-
News & Updates
strong-admin
April 4, 2014
Scoliosis
Scoliosis Affects the Entire Body
Scoliosis affects the entire skeletal system including the spine, ribs, and pelvis. It impacts upon the brain and central nervous system and affects the body’s hormonal and digestive systems. It can deplete the body’s nutritional resources and damage its major organs including the heart and lungs.
Some factors that can cause scoliosis include: cerebral palsy, birth defects, muscular dystrophy and Marfan syndrome. However, 80% of scoliosis is idiopathic (unknown in origin).
According to the Scoliosis Care Foundation, one in nine females and a smaller percentage of males have some sign of scoliosis. Approximately 4% of the general population is affected. While the average patient is between 10-15 years of age, many adults suffer from this disease as well.
Conditions arising as a result of scoliosis include rib deformity, shortness of breath, digestive problems, chronic fatigue, acute or dull back pain, leg, hip, and knee pain, acute headaches, mood swings, and menstrual disturbances.
Scoliosis is a progressive condition that can continue to progress even after skeletal maturity. Millions of scoliosis sufferers are routinely misinformed about the accelerating nature of their spinal curvature progression.
April 4, 2014
Treatment for scoliosis
Treatment for scoliosis recommendations are based on comprehensive examinations which include; Neurologic, Orthopedic, Radiologic, and Postural findings.
Age, growth and bone maturity are not necessarily limiting factors for most patients. The Spinecor Brace and Schroth Exercise Program are effective in both Children and Adults with Scoliosis. Expected outcomes vary depending upon the individual patient more than their age or growth potential.
Treatment for Scoliosis without the use of bracing- Scoliosis bracing continues to be controversial due to its difficult nature and long course of treatment, however, the use of scoliosis braces has been shown to alter the natural history of the disease. Therefore, bracing is a usefull tool in the non-surgical management of scoliosis, and the question is not if bracing should be used, but what type of brace is best. Chiropractic and other non-bracing proceedures may serve to increase flexibility and may even create a transient reduction in the measurement of the curvature, however, they have not been shown to make a lasting impact on the natural history of the disease. Therefore we continue to recommend the spinecor scoliosis brace for Juvienial and Adolescent Idiopathic Scoliosis in conjunction with the Schroth Method exercises.
In Adult scoliosis, whether it be De-Novo or long standing in nature, spinal degeneration and postural weakness make the Spinecor brace a vital component to treatment success. Patients who are able to make lifestyle changes necessary to exercise 4-6 hours per day may not need the Spinecor brace, but the majority of adults with scoliosis must continue to work and cannot feasibly make corrections to their spine without the use of a postural support such as Spinecor.
Internal Representation of Self – Postural re-education is a necessary part of the rehabilitation process. Through conscious posturing exercises and walking, patients are taught to become aware of body position and can consciously reduce the effects of sitting, slouching and habituatal movement on Scoliosis.
Neurological Influence on Posture – When neurological dysfunction arises from central origin, active inhibition of muscle compartments is lost, this over activity can be reduced with muscle stretching techniques which include Chiropractic Neurology procedures.
Muscle Activation Strategies– With improved sense of self, and reduced neurological interference, retraining of muscle activation patterns is more probable. See below for more…
1. Vestibular Rehabilitation For Scoliosis: Many studies identify vestibular and oculomotor dysfunction in the majority of patients with Scoliosis. Habituation training and vestibular therapy exercises may be appropriate for patients with vestibular involvement in their Scoliosis. Therapies and exercises to improve the central neurological controls of posture may include vestibular and oculomotor rehabilitation. Following a functional neurological evaluation, including the use of state-of-the-art diagnostic equipment to evaluate vestibular function, a neurological retraining program is designed for patients individually.
2. Exercise Physiology Training For Scoliosis: Procedures utilized may include: Respiratory exercises using trunk positioning, sustained contraction exercises to influence muscle fiber changes, Active Isolated Stretch and Myofascial Release Technique for active inhibition of shortened musculature, Dynamic Vestibulospinal Rehabilitation training may also be appropriate to influence new muscle recruitment patterns.
3. Dynamic Flexion Distraction of the Spine: The flexion distraction table is a special device designed to stretch the spine through a gentle, non-force procedure. It is mostly recommended in cases with pain and diminished ranges of motion. Spinal rotation and lateral flexion activity is often restricted and may lead to abnormal muscle recruitment strategies. Spinal curvatures can be manually stretched while bringing the patient through a corrective movement strategy. Correct coupled motion is therapeutic and creates feedback though spinal sensory system. These procedures are designed to allow for greater correction with the use of a dynamic truncal orthosis.
5. Nutritional Support: Exercise and physiotherapy procedures create free radicals which may be effectively neutralized with certain nutritional supplements. Postural tone may also be improved with the use of certain coenzymes and fatty acids. Many patients with Scoliosis have digestive problems and may respond well to digestive enzyme support.
April 4, 2014
“My doctor told me to wait and see.”
 “My child was diagnosed with scoliosis by our pediatrician, she referred us to an Orthopedist, but he said not to worry and come back in 6 months.”
“My child was diagnosed with scoliosis by our pediatrician, she referred us to an Orthopedist, but he said not to worry and come back in 6 months.”April 4, 2014
Scoliosis Affects the Entire Body
Scoliosis Affects are on the Entire Body
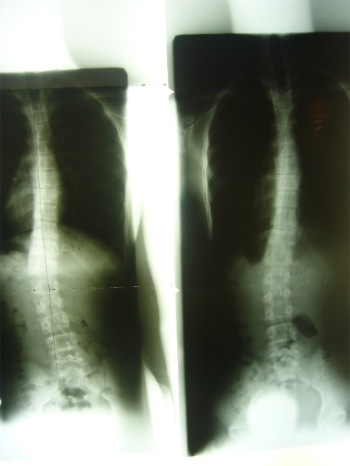
Scoliosis is generally viewed as a lateral curvature of the spine with an axial twist that causes a distortion of the ribs. Current research shows that idiopathic scoliosis is a multifaceted disease that compromises five of the body’s systems: digestive, hormonal, muscular, osseous (bones), and neurologic.
Scoliosis affects the entire skeletal system including the spine, ribs, and pelvis. It impacts upon the brain and central nervous system and affects the body’s hormonal and digestive systems. It can deplete the body’s nutritional resources and damage its major organs including the heart and lungs.
Some factors that can cause scoliosis include: cerebral palsy, birth defects, muscular dystrophy and Marfan syndrome. However, 80% of scoliosis is idiopathic (unknown in origin).
According to the International Scoliosis Society, one in nine females and a smaller percentage of males have some sign of scoliosis. Approximately 4% of the general population is affected. While the average patient is between 10-15 years of age, many adults suffer from this disease as well.
Conditions arising as a result of scoliosis include rib deformity, shortness of breath, digestive problems, chronic fatigue, acute or dull back pain, leg, hip, and knee pain, acute headaches, mood swings, and menstrual disturbances.
Scoliosis is a progressive condition that can continue to progress even after skeletal maturity. Millions of scoliosis sufferers are routinely misinformed about the accelerating nature of their spinal curvature progression.
April 4, 2014
Scoliosis Systems Patient Avoids Surgery
 |
 |
 |
| 36° Initial | 2 in brace 30° | 34° 2 + yrs out of brace |