-
News & Updates
Marc Lamantia D.C.
May 25, 2017
Scoliosis, Osteoporosis and Vertigo in Clinical Practice
Scoliosis, Osteoporosis and Vertigo in Clinical Practice
Do you have one or more of the following; Scoliosis, Osteoporosis or Vertigo? Clinicians and Researchers have long reported that all three of these conditions can occur simultaneously. And now, new research may answer at least in part why patients with Scoliosis also have Osteoporosis and Vertigo.
May 16, 2017
Scoliosis Progression linked to Adolescent Version of Osteoporosis
Link Between Scoliosis Progression And Osteoporosis
It’s not surprising that osteoporosis has been found to be a risk factor for progression in adults with scoliosis, so it should also stand to reason that similar bone mineral deficiency can lead to scoliosis progression in adolescents.
Increased Risk Factor In Scoliosis Progression In Adolescents Linked To Similar Condition
The study entitled Osteopenia: A New Prognostic Factor of Curve Progression In Adolescent Idiopathic Scoliosis showed that adolescent girls with scoliosis were at greater risk for progression when they concurrently had osteopenia.
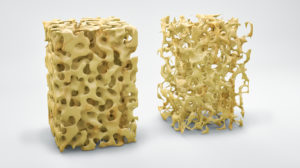
Osteopenia is the thinning of bone mass and is often considered the precursor to the more severe condition of osteoporosis that usually occurs later in life. Osteoporosis aka “Fragile Bone Disease” is characterized by a loss of bone mass caused by a deficiency in calcium, vitamin D, magnesium and other vitamins and minerals and is usually only thought to problem associated with menopause.
In this study researchers evaluated the bone mineral density (BMD) in the spine and hips of 324 adolescent girls with scoliosis. What they found was a correlation between a diminished BMD in girls with scoliosis to an increased likelihood of progression of their curvatures. The suggestion that diminished bone mineral density is a risk factor for progression of a scoliosis also does not come as a surprise.
What was surprising was the high percentage of adolescents with scoliosis that were also found to have osteopenia. Researchers estimated that as many 38% of young girls with scoliosis also have osteopenia, putting patients in this group at a significantly increased risk for curvature progression!

Table V. In this table researchers divided the girls into two groups based on the progression of their curves:
Group A. – Patients With Stable Curves
Group B. – Patients with Curve Progression
What they found was that over time the group that had progression of their curves also had a greater loss in bone density. Thus the evidence is clear that lower bone mineral density is a risk factor for progression.

Evaluation and Treatment Recommendations in Light of Study
As a result, doctors with Scoliosis Systems now recommend a Bone Density test (DEXA or DXA Scan) and a blood test for Vitamin D and Calcium Deficiencies to rule out this important risk factor for scoliosis progression in Adolescence. The results can be important in making dietary and supplement recommendations for those showing signs of osteopenia.
The authors also identified other risk factors for scoliosis progression which included a delayed onset of the menses. The research shows Ammenorhea and scoliosis progression are linked. The findings from both studies confirm hormones and bone health are directly related. Estrogen and Testosterone must be in balance for the menses to occur and continue regularly. Researchers routinely find testosterone to be in high concentrations in scoliosis adolescents, which leads to the interruption of the menses and the normal bone density.
Scoliosis tends to progress the greatest during the times of the increased metabolic activity such as the major growth spurt that occurs at the onset of puberty, also during pregnancy and menopause.
Weight bearing activity improves bone density, however this proves less effective in scoliosis patients. One reason this may be true is due to the asymmetrical loading to the bones in scoliosis curvatures.
Marc J. Lamantia DC
March 1, 2016
Neuroskeletal Management of Scoliosis-Certificate Program for D.C.s
2 Hour Live Webinar – 2CE
Introduction to Neuro-skeletal Scoliosis ($50)
-
Learn the 5 Mistakes Chiropractors Make when treating Scoliosis
- Ask live questions about cases you currently are seeing
Co-Sponsor; New York Chiropractic College
Give us your Contact Information if you would like to receive alerts about Seminar Dates and Times
September 22, 2015
A Randomized Controlled Study of the Natural History of Idiopathic Scoliosis vs SpineCor Treatment
 A research study at Sainte Justine’s University Children’s Hospital & Research Center in Montreal Canada was led by two prominent orthopedic surgeons, Dr. Christine Coillard and Dr. Charles Rivard to examine the differences in outcomes between adolescents with scoliosis that were not treated at all for their scoliosis and those treated with SpineCor.
A research study at Sainte Justine’s University Children’s Hospital & Research Center in Montreal Canada was led by two prominent orthopedic surgeons, Dr. Christine Coillard and Dr. Charles Rivard to examine the differences in outcomes between adolescents with scoliosis that were not treated at all for their scoliosis and those treated with SpineCor.
Scoliosis Natural Progression vs SpineCor from Brett Diaz on Vimeo.
The study titled A Prospective Randomized Controlled Trial of the Natural History of Idiopathic Scoliosis versus Treatment with the Spinecor Brace divided a group of 68 teens who had been diagnosed with idiopathic scoliosis who’s curves were between 15° to 30° and were at high risk for progression into 2 groups. The Treatment Group were fitted for SpineCor braces while the Control Group received the common recommendation of just “Watch & Wait” and do nothing to treat the scoliosis. This allowed them to compare the natural history of scoliosis progression in cases that had gone untreated and compare the outcome to cases in the other group that had received SpineCor treatment.
Patient’s were considered to be at “High Risk” for progression if they had any of the following risk factors:
• A family history of scoliosis
• Early onset of a curve
• Late onset of puberty
• They’ve already shown some progression in their curves
Researchers evaluated the differences in outcomes over a 5 year period between the 2 groups and at the end of the 5 year study the data showed that 50% of the SpineCor Group had improvement in their curves compared to only 9.5% in the control population.
It also found that the untreated group had nearly double the rate of scoliosis progression vs. the SpineCor treated group. In fact because the parameter’s of the study that would not allow for children who showed progression to go untreated it removed them from the control group if they had a progression of more than 5° they would be removed from the study and provided with treatment.
This study showed that for children with risk factors for progression were left untreated then the natural progression of scoliosis is likely to get worse in approximately 50% of these patients.
While those treated with the SpineCor brace were able to significantly reduce the probability of the progression, 73.1% of the time in early idiopathic scoliosis compared with its natural history.
Extrapolation of the study data showed that had those untreated control subjects patients stayed in the study that the overall progression of the group would have be around 75%. That’s nearly three times the rate of scoliosis progression compared to those patients treated with SpineCor!
The long term results with SpineCor treatment showed that 73.1% of patients had continued stabilization or further reduction of their curve after stopping treatment and was maintained over the long term. This makes SpineCor an effective long-term treatment for scoliosis that is best provided early on, when the curve is most correctable.
August 28, 2015
The Role of Muscles In Stabilization of the Spine In Scoliosis Rehabilitation

In scoliosis specific exercise there are 2 different camps of thought when it comes to strengthening weakened muscles to help stabilize the spine. One camp believes that only the deep postural muscles of the trunk that directly attach to the spine are necessary to activate, the other camp feels that both the deep postural muscles and the more superficial muscles that attach the spine to the upper and lower lower extremities are important to activate.
A study done presented in the Spine Journal in 2004 titled Determining the Stabilizing Role of Individual Torso Muscles During Rehabilitation Exercises studied individual lumbar muscles in order to assess their potential stabilizing role by comparing and recording the Electromyography (EMG) activity produced by different skeletal muscles in both the deep and superficial layers of the spine.
The results of their study revealed that spinal stability was not dominated by any single muscle group in the spine. Instead it appeared that all the muscles in the spine dynamically changed in their level of support to the spine as the tasks the body performed altered the position of the body as controlled by the nervous system.
Based on these findings they concluded that the best strategy for enhancing motor patterns of muscles in the spine to promote stability of the spine would be best to activate the multitude of muscles involved in the action then just targeting a few of the deep postural muscles.
This supports the long held belief of the Schroth Method that it’s important to take a “Whole Body” approach to rehab rather than artificially restricting the focus to only one area of the spine.