-
News & Updates
Scoliosis
April 4, 2014
Adult Spinecor Brace
Spinecor for Adult Scoliosis Click here |
| Should Adults With Scoliosis Use the Adult Spinecor Brace?On April 17 2009, the Adult spinecor Brace for Scoliosis was made available by Dr. Marc Lamantia and Dr. Gary Deutchman in all 14 offices throughout the United States. The new adult Spinecor brace design is more comfortable and hides even better under the clothes. Although Dr. Lamantia and Dr. Deutchman did the original research on adults and Spinecor, and have been fitting adults with scoliosis since 2004, the Spinecorporation now recommends spinecor for adult use.
For more information on the Spinecor brace for adults with scoliosis call 1-800-281-5010 or email us by clicking on the link below. Although the Spinecor brace was originally developed for adolescent idiopathic scoliosis treatment, clinical uses for adults with scoliosis, patients with kyphosis and non-idiopathic scoliosis are encouraging. Adults with scoliosis are routinely referred for adult Spinecor bracing to our New York, Chicago, Atlanta, North Carolina, Denver, Buffalo, St. Louis, Tampa, Ft Lauderdale, Roswell (GA), Washington State, Dallas, Houston, Los Angeles, San Francisco and the Inland Empire (CA) offices. Since the first adult fitting in the Spinecor brace, Drs. Deutchman and Lamantia has fitted over 1000 patients with all types of curvatures. Adults with scoliosis often experience pain relief immediately when the Spinecor brace if fitted appropriately. Due to the nature of the adult spine with scoliosis, different Spinecor brace configurations were developed to successfully manage adult patients. Dr. Deutchman and Lamantia are unmatched in this area of expertise. Studies show adult scoliosis to be potentially progressive in nature and to be a major contributor to chronic pain, radiculopathy and neurogenic claudication. Due to the abnormal posture and muscle recruitment patterns associated with adult scoliosis, adult Spinecor bracing should be supported with specialized physiotherapy programs. Unlike a rigid brace, the Spinecor brace uses a rotational 3D Corrective Movement which has been shown to be effective in reducing scoliosis curvatures in adolescents and adults. The Spinecor brace is a dynamic system of elastic bands which uses gentle forces to change posture and movement patterns over time. It can easily be worn under the clothes, during exercise and at work. Adult scoliosis management differs from adolescent scoliosis treatments due to the long standing dysfunction of the motion segments of the spine and associated ligament degeneration. This may lead to subluxation (misalignment of the vertebra) and further degenerative change to both bone and soft tissues. Often, adult scoliosis treatment can be successful if the patient can tolerate the Spinecor brace. Careful evaluation and fitting procedures are necessary to ensure adults do not experience exacerbations of pain and nerve irritation. Spinecor brace research shows adults can achieve scoliosis curvature reduction despite reaching maximal bone maturity. Due to the fact that spinal deformities associated with scoliosis are not entirely from bone deformity, but include influences from ligament, disc and muscle function. Our adult Spinecor patients routinely respond in our program which may include Schroth Exerices and chiropractic care. Results vary between individuals. Chiropractic management is recommended when subluxations are detected. For more information contact one of our doctors. Video Testimonials of Adult Spinecor brace patients Video Testimonials of Spinecor brace patients References Natural history of the aging spine., Benoist M, Eur Spine J. 2003 Oct;12 Suppl 2:S86-9. Epub 2003 Sep 05. Orthopaedic Surgery Unit, Department of Rheumatology, Hopital Beaujon, 100 Bd du Gal Leclerc, 92110, Clichy, France. [email protected] Spinal mobility and EMG activity in idiopathic scoliosis through dynamic lateral bending tests. Stud Health Technol Inform. 2002;91:130-4.,Ciolofan OC, Aubin CE, Mathieu PA, Beausejour M, Feipel V, Labelle H. Sainte-Justine Hospital, 3175 Cote Ste-Catherine Rd, Montreal, H3T 1C5, Canada. Biomechanical factors affecting progression of structural scoliotic curves of the spine. Lupparelli S, Pola E, Pitta L, Mazza O, De Santis V, Aulisa L. Stud Health Technol Inform. 2002;91:81-5 Degeneration of the human lumbar spine ligaments. An ultrastructural study. Yahia H, Drouin G, Maurais G, Garzon S, Rivard CH.Biomedical Engineering Institute, Faculty of Medicine, Montreal, Canada. Pathol Res Pract. 1989 Apr; 184(4): 369-75. Natural history of the aging spine., Benoist M, Eur Spine J. 2003 Oct;12 Suppl 2:S86-9. Epub 2003 Sep 05. Orthopaedic Surgery Unit, Department of Rheumatology, Hopital Beaujon, 100 Bd du Gal Leclerc, 92110, Clichy, France. [email protected] Vestibular mechanisms involved in idiopathic scoliosis, Arch Ital Biol. 2002 Jan;140(1):67-80. |
| Contact: Gary A. Deutchman, D.C. and Marc J. Lamantia M.S.,D.C.1-800-281-5010mailto:[email protected] |
April 4, 2014
NEWS-8/6/10 MRI Replaces X-ray in Scoliosis Care.
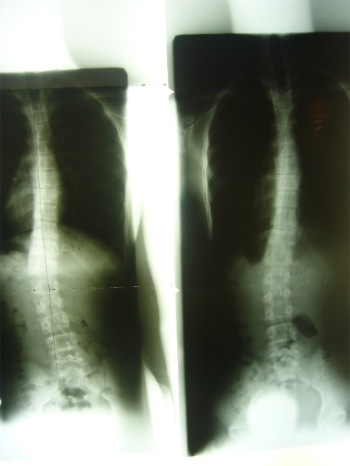
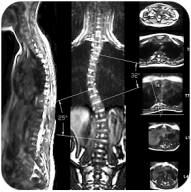 The first completely non-radiation management for Scoliosis is now available. MRI has no known side effects and can now be used to evaluate scoliosis both in and out of braces. The New Scoliosis Coil developed by Fonar MRI is now being used in San Jose CA and New York City. “This is a milestone in the clinical management of scoliosis”, according to Dr. Gary Deutchman, co-founder of Scoliosis Systems LLP.
The first completely non-radiation management for Scoliosis is now available. MRI has no known side effects and can now be used to evaluate scoliosis both in and out of braces. The New Scoliosis Coil developed by Fonar MRI is now being used in San Jose CA and New York City. “This is a milestone in the clinical management of scoliosis”, according to Dr. Gary Deutchman, co-founder of Scoliosis Systems LLP.
X-ray exposure in the management of Scoliosis has long been a concern.. “Although we have always used gonadal and breast shielding, we are so pleased to be the first Scoliosis Clinic in the World to offer MR Imaging as a viable alternative to x-ray”, says Dr. Marc Lamantia.
Scoliosis affects nearly 1 million Americans each year. Newer bra
ce technologies and advances in rehabilitation techniques have given millions of adults and children an alternative to surgery and rigid braces. With more people seeking treatment in adulthood, the need for safer imaging techniques has spurred inventions like Rastersteropgraphy, and now Scoliosis sensitive MRI. “MRI is a safe and cost effective way to monitor scoliosis in both children and adults. I hope more clinicians will offer MRI to their patients, for now, there are a handfull of us pionnering change.”, says Dr. Deutchman.
April 4, 2014
Scoliosis
Scoliosis Affects the Entire Body
Scoliosis affects the entire skeletal system including the spine, ribs, and pelvis. It impacts upon the brain and central nervous system and affects the body’s hormonal and digestive systems. It can deplete the body’s nutritional resources and damage its major organs including the heart and lungs.
Some factors that can cause scoliosis include: cerebral palsy, birth defects, muscular dystrophy and Marfan syndrome. However, 80% of scoliosis is idiopathic (unknown in origin).
According to the Scoliosis Care Foundation, one in nine females and a smaller percentage of males have some sign of scoliosis. Approximately 4% of the general population is affected. While the average patient is between 10-15 years of age, many adults suffer from this disease as well.
Conditions arising as a result of scoliosis include rib deformity, shortness of breath, digestive problems, chronic fatigue, acute or dull back pain, leg, hip, and knee pain, acute headaches, mood swings, and menstrual disturbances.
Scoliosis is a progressive condition that can continue to progress even after skeletal maturity. Millions of scoliosis sufferers are routinely misinformed about the accelerating nature of their spinal curvature progression.
April 4, 2014
Treatment for scoliosis
Treatment for scoliosis recommendations are based on comprehensive examinations which include; Neurologic, Orthopedic, Radiologic, and Postural findings.
Age, growth and bone maturity are not necessarily limiting factors for most patients. The Spinecor Brace and Schroth Exercise Program are effective in both Children and Adults with Scoliosis. Expected outcomes vary depending upon the individual patient more than their age or growth potential.
Treatment for Scoliosis without the use of bracing- Scoliosis bracing continues to be controversial due to its difficult nature and long course of treatment, however, the use of scoliosis braces has been shown to alter the natural history of the disease. Therefore, bracing is a usefull tool in the non-surgical management of scoliosis, and the question is not if bracing should be used, but what type of brace is best. Chiropractic and other non-bracing proceedures may serve to increase flexibility and may even create a transient reduction in the measurement of the curvature, however, they have not been shown to make a lasting impact on the natural history of the disease. Therefore we continue to recommend the spinecor scoliosis brace for Juvienial and Adolescent Idiopathic Scoliosis in conjunction with the Schroth Method exercises.
In Adult scoliosis, whether it be De-Novo or long standing in nature, spinal degeneration and postural weakness make the Spinecor brace a vital component to treatment success. Patients who are able to make lifestyle changes necessary to exercise 4-6 hours per day may not need the Spinecor brace, but the majority of adults with scoliosis must continue to work and cannot feasibly make corrections to their spine without the use of a postural support such as Spinecor.
Internal Representation of Self – Postural re-education is a necessary part of the rehabilitation process. Through conscious posturing exercises and walking, patients are taught to become aware of body position and can consciously reduce the effects of sitting, slouching and habituatal movement on Scoliosis.
Neurological Influence on Posture – When neurological dysfunction arises from central origin, active inhibition of muscle compartments is lost, this over activity can be reduced with muscle stretching techniques which include Chiropractic Neurology procedures.
Muscle Activation Strategies– With improved sense of self, and reduced neurological interference, retraining of muscle activation patterns is more probable. See below for more…
1. Vestibular Rehabilitation For Scoliosis: Many studies identify vestibular and oculomotor dysfunction in the majority of patients with Scoliosis. Habituation training and vestibular therapy exercises may be appropriate for patients with vestibular involvement in their Scoliosis. Therapies and exercises to improve the central neurological controls of posture may include vestibular and oculomotor rehabilitation. Following a functional neurological evaluation, including the use of state-of-the-art diagnostic equipment to evaluate vestibular function, a neurological retraining program is designed for patients individually.
2. Exercise Physiology Training For Scoliosis: Procedures utilized may include: Respiratory exercises using trunk positioning, sustained contraction exercises to influence muscle fiber changes, Active Isolated Stretch and Myofascial Release Technique for active inhibition of shortened musculature, Dynamic Vestibulospinal Rehabilitation training may also be appropriate to influence new muscle recruitment patterns.
3. Dynamic Flexion Distraction of the Spine: The flexion distraction table is a special device designed to stretch the spine through a gentle, non-force procedure. It is mostly recommended in cases with pain and diminished ranges of motion. Spinal rotation and lateral flexion activity is often restricted and may lead to abnormal muscle recruitment strategies. Spinal curvatures can be manually stretched while bringing the patient through a corrective movement strategy. Correct coupled motion is therapeutic and creates feedback though spinal sensory system. These procedures are designed to allow for greater correction with the use of a dynamic truncal orthosis.
5. Nutritional Support: Exercise and physiotherapy procedures create free radicals which may be effectively neutralized with certain nutritional supplements. Postural tone may also be improved with the use of certain coenzymes and fatty acids. Many patients with Scoliosis have digestive problems and may respond well to digestive enzyme support.
April 4, 2014
“My doctor told me to wait and see.”
 “My child was diagnosed with scoliosis by our pediatrician, she referred us to an Orthopedist, but he said not to worry and come back in 6 months.”
“My child was diagnosed with scoliosis by our pediatrician, she referred us to an Orthopedist, but he said not to worry and come back in 6 months.”